Learning Objectives
3 objectivesBy the end of this note, you should be able to:
- Analyse quantitative illness and mortality data, distinguishing correlation from causation.
- Evaluate sample selection, sample size, validity and reliability of risk-factor studies.
- Explain why people’s perception of risk differs from actual lifestyle and dietary risk.
Analysing Health Risk Data and Causation
A health risk is the probability that an individual will develop a disease or suffer harm from a specific factor over time.
Scientists quantify illness using morbidity rates [the number of disease cases in a population] and mortality rates [the number of deaths per population per year]. These rates allow valid comparisons between groups exposed to different lifestyle factors. For example, mortality from coronary heart disease (CHD) can be compared between smokers and non-smokers, or between low-fat and high-fat diet groups.
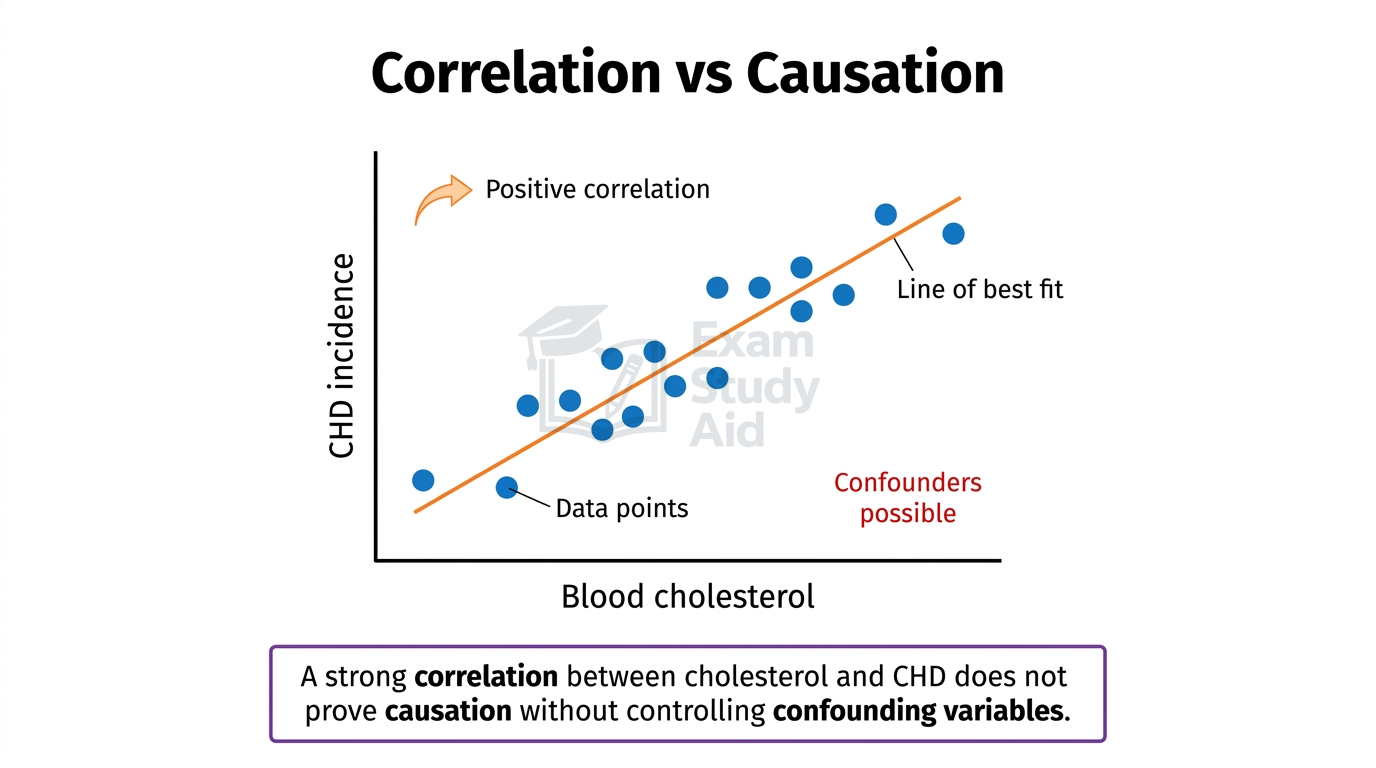
When two variables change together, they show a correlation. This does not always mean that one variable causes the other. Causation only exists when a change in one variable directly produces the change in another. To establish causation, scientists must rule out confounding variables [additional factors that could explain the relationship].
Consider blood cholesterol and CHD. People with high blood cholesterol show higher rates of CHD, which is a correlation. However, those individuals may also smoke, eat poorly, exercise less, or have a genetic predisposition. Each confounder could partly explain the disease pattern.
Studies often produce conflicting evidence. One study may report that moderate alcohol intake protects the heart, while another finds no benefit. Differences arise from sample populations, study lengths, methods of measurement, and how confounders are handled. Strong conclusions therefore require many independent studies showing consistent findings.
MisconceptionStudents often write that high cholesterol “causes” CHD when given correlation data alone. Examiners require evidence from controlled studies before any causal claim can be made. Correlation by itself is never sufficient proof.
Exam TipAlways check whether confounding variables have been excluded before claiming causation.
Evaluating Study Design for Risk Factors
The strength of any conclusion about a risk factor depends on how the study is designed. Examiners expect candidates to evaluate four things: sample selection, sample size, validity, and reliability.
Sample selection must produce a group representative of the wider population. A sample of only middle-aged men cannot be used to draw conclusions about women or younger groups. Researchers often use random sampling or stratified sampling [dividing the population into subgroups before sampling] to reduce selection bias.
Sample size strongly affects the weight given to the conclusion. A small sample is easily influenced by chance variation and produces noisy averages. Larger samples produce more reliable means and detect smaller true effects with greater confidence.
A study is valid if it measures what it claims to measure, and is reliable if repeating it produces consistent results. The two ideas are easily confused but tested differently.
| Term | Meaning | Improved By |
|---|---|---|
| Valid | Measures what it claims to measure | Tightly controlling all variables; using accurate equipment |
| Reliable | Produces consistent results when repeated | Using large samples; repeating the study; standardising methods |
Other examinable features of strong study design include:
- Using a control group not exposed to the risk factor.
- Following participants over a long period (longitudinal study).
- Recording lifestyle data accurately at regular intervals.
- Statistically adjusting for known confounding variables.
- Reducing observer bias through blinding [where participants or researchers do not know group allocations].
Examiner InsightWhen asked to “evaluate” a study, candidates often only describe what was done. The mark requires a judgement: which features strengthen the conclusion, which weaken it, and why. State both, with reasons.
Exam TipUse linking phrases like “this strengthens the validity because…” to score evaluation marks.
Risk Perception vs Actual Risk
People often perceive health risks very differently from their actual statistical risk. This mismatch affects whether individuals modify their behaviour, even when reliable data is available.
Several psychological factors distort risk perception:
- Familiarity: well-known risks (driving, eating fast food) are underestimated because they feel routine.
- Novelty: new or unfamiliar risks (a new disease, a rare food additive) are overestimated because they feel threatening.
- Voluntary control: chosen risks (smoking, sunbathing) feel less dangerous than imposed ones (air pollution).
- Personal experience: if a relative lived to ninety despite smoking, an individual may dismiss the population risk.
- Optimism bias: people tend to believe they are personally less likely than others to suffer harm.
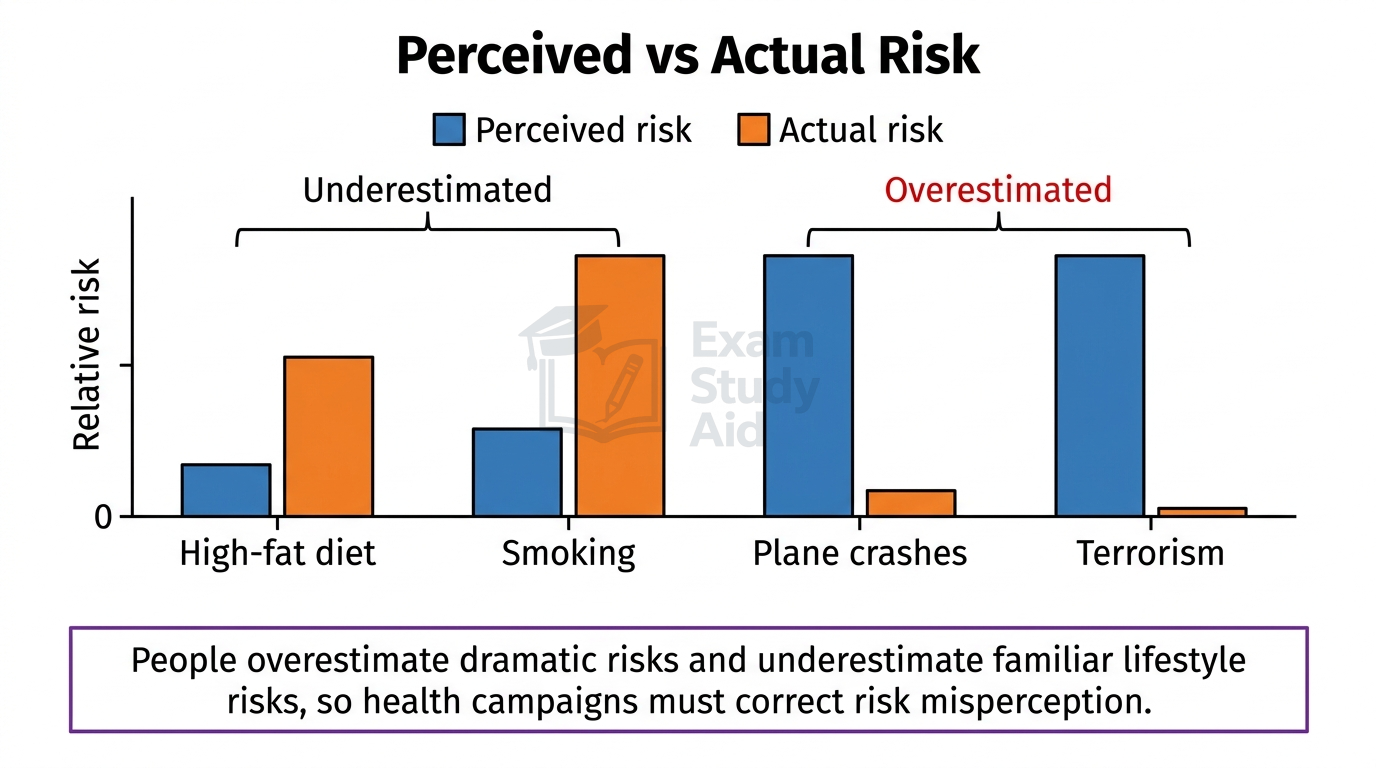
- Media coverage: dramatic but rare events (terrorism, plane crashes) receive heavy reporting, inflating perceived risk.
For coronary heart disease specifically, the gap between perceived and actual risk is large. Many people underestimate the contribution of saturated fat, trans fat, and salt in their everyday diet. Long-term harm from being overweight or sedentary is also frequently dismissed as future, not current, risk. By contrast, people often overestimate the protection offered by occasional exercise or “healthy” foods marketed as low-fat.
These biases matter because individuals must accept their own risk before they will modify diet, smoking, or activity levels. Effective public health campaigns therefore aim to correct misperception, not just present statistics.
QUICK RECAP
Key Points
- Risk = probability of harm or disease occurring.
- Morbidity rate = cases of illness per population.
- Mortality rate = deaths per population per year.
- Correlation = two variables changing together.
- Causation = one variable directly producing change in another.
- Correlation does not prove causation; confounders may explain results.
- Conflicting evidence arises from sample, design, and measurement differences.
- Sample selection must be representative, often via random/stratified sampling.
- Larger samples reduce chance variation and increase reliability.
- Valid = measures what it claims; reliable = consistent on repetition.
- Strong studies use control groups, long follow-up, and confounder adjustment.
- Familiar/voluntary/slow-developing risks are underestimated.
- Novel/involuntary/dramatic risks are overestimated.
- People underestimate dietary and sedentary lifestyle risks for CHD.
- Optimism bias makes individuals dismiss population statistics.
CAN I…? PROGRESS CHECK
Self-Assessment
- Define risk, morbidity rate and mortality rate?
- Distinguish correlation from causation, giving an example?
- Identify confounding variables in a CHD risk study?
- Explain why two studies on the same factor may give conflicting evidence?
- Evaluate the validity and reliability of a given study design?
- Justify the importance of representative sample selection and sample size?
- List the psychological factors that distort risk perception?
- Explain why dietary risks for CHD are commonly underestimated?