Learning Objectives
5 objectivesBy the end of this note, you should be able to:
- Analyse data on health significance of blood cholesterol, HDL and LDL levels
- Evaluate evidence linking blood cholesterol to cardiovascular disease
- Explain how diet, exercise and smoking affect coronary heart disease risk
- Describe obesity indicators including body mass index and waist-to-hip ratio
- Compare benefits and risks of antihypertensives, statins, anticoagulants and platelet inhibitors
Blood Cholesterol, HDLs and LDLs
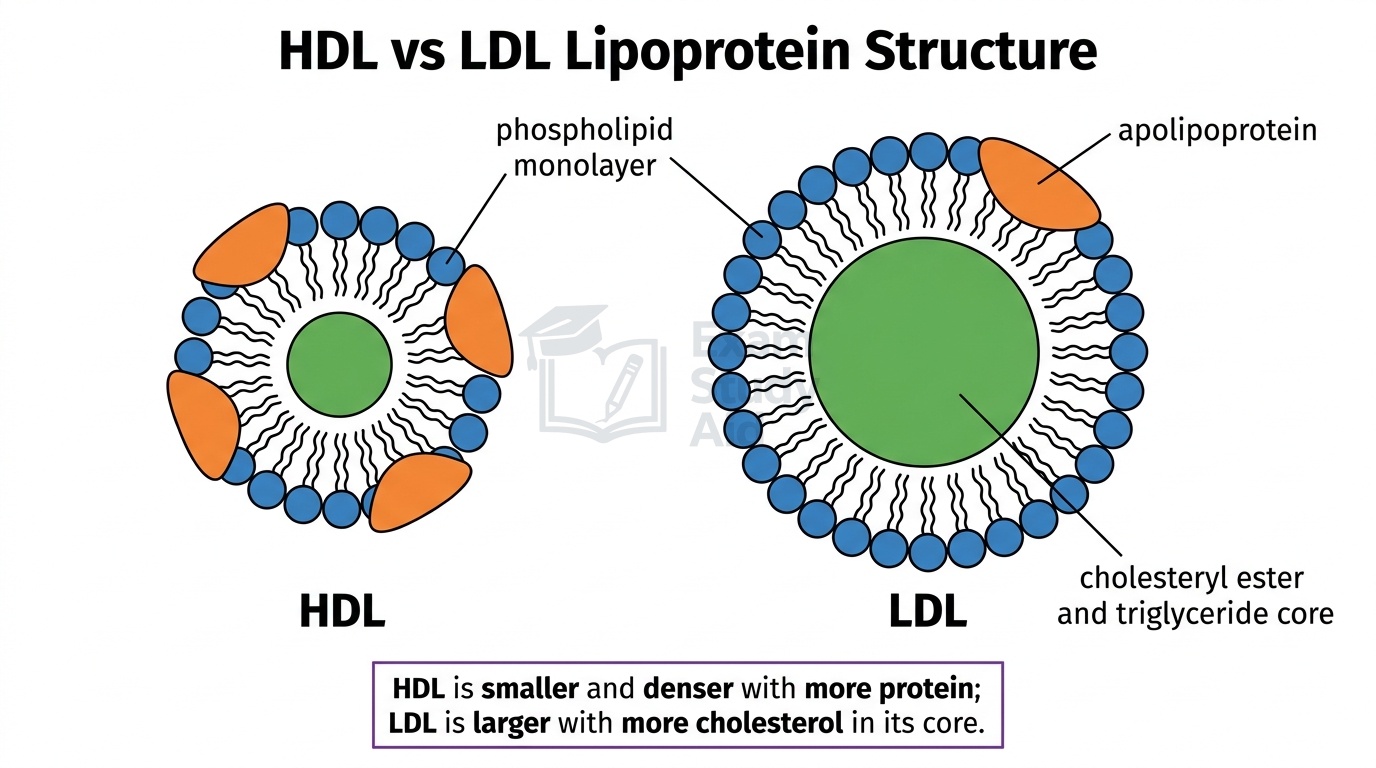
Cholesterol is a lipid made mainly in the liver and absorbed from animal foods, and it cannot dissolve in blood plasma. The body solves this by attaching cholesterol to proteins, forming lipoproteins that carry it through the bloodstream.
There are two main types you must know. High-density lipoproteins (HDLs) contain more protein and less cholesterol, giving them a higher density. They transport cholesterol from body tissues back to the liver for breakdown and excretion. For this reason, HDLs are often called “good cholesterol”.
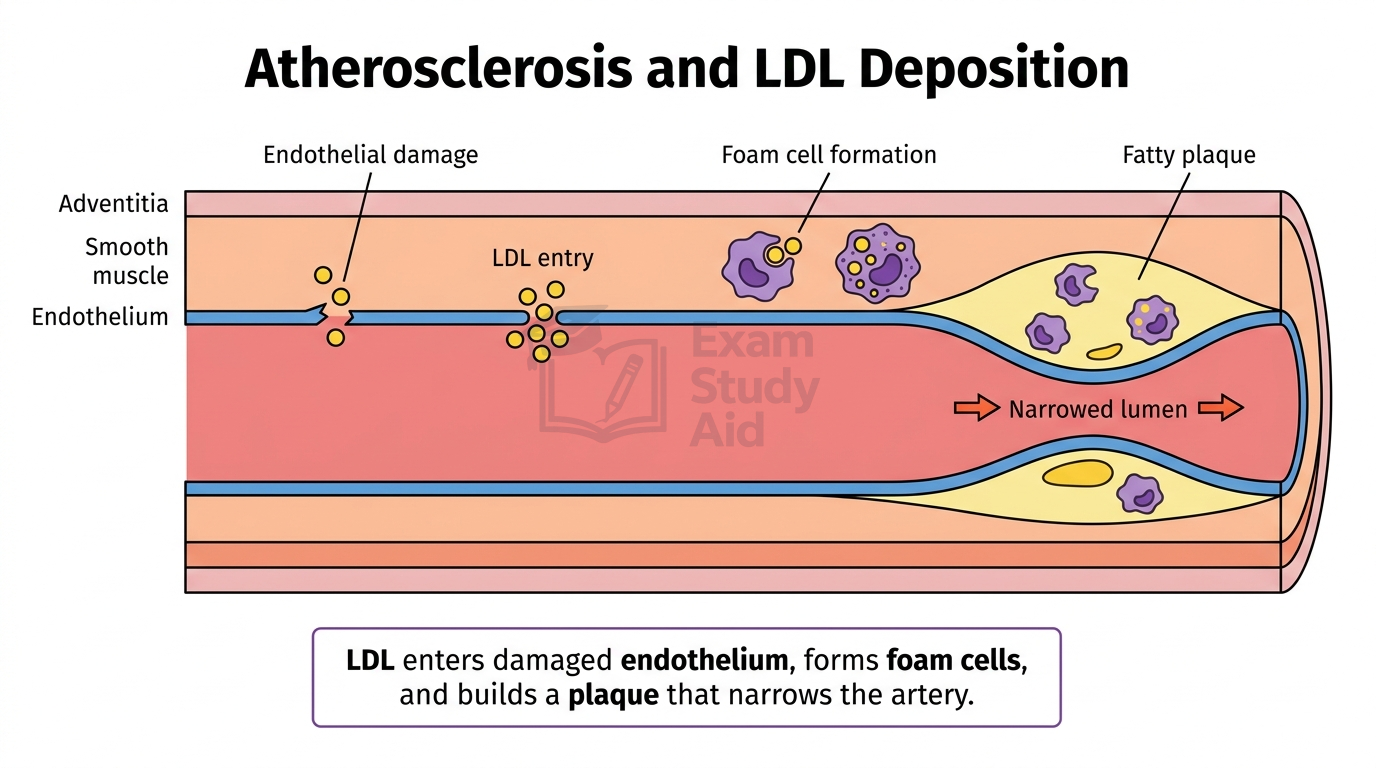
Low-density lipoproteins (LDLs) contain more cholesterol and less protein, giving them a lower density. They carry cholesterol from the liver to body cells. When blood LDL levels are high, LDLs can deposit cholesterol inside artery walls, contributing to atherosclerosis. This is why LDLs are often called “bad cholesterol”.
When analysing health data, three values matter most for predicting cardiovascular disease (CVD) risk:
| Measurement | Healthy guideline (UK) | Health significance |
|---|---|---|
| Total cholesterol | Below 5.0 mmol/dm³ | Higher levels increase CVD risk |
| LDL cholesterol | Below 3.0 mmol/dm³ | Strong link to atherosclerosis |
| HDL cholesterol | Above 1.0 mmol/dm³ (men), 1.2 (women) | Higher levels are protective |
A high HDL:LDL ratio is more protective than just a low total cholesterol value. Two people can share the same total cholesterol yet have very different CVD risks depending on this ratio.
MisconceptionStudents often write that HDL and LDL are types of cholesterol. They are not. HDL and LDL are lipoprotein carriers that transport cholesterol through the bloodstream. Only the transport particle differs between them.
Exam TipAlways write “HDL transports cholesterol”, never “HDL is cholesterol”.
Evidence Linking Cholesterol to CVD
A causal relationship between high blood cholesterol, especially LDL, and CVD has been established through multiple lines of evidence rather than any single study.
Large-scale epidemiological studies show that populations with higher average blood cholesterol have higher rates of CVD. The Framingham Heart Study (running since 1948) followed thousands of participants and found that CVD risk rose steadily with rising LDL cholesterol. This shows a dose-response relationship, where greater exposure produces greater harm.
Genetic evidence comes from people with familial hypercholesterolaemia, an inherited condition where LDL receptors are faulty. These individuals have very high LDL from birth and develop atherosclerosis decades earlier than the general population. This shows that high LDL itself causes CVD, not just an unhealthy lifestyle.
Animal studies support this further. Rabbits fed high-cholesterol diets develop fatty deposits in their arteries similar to human atherosclerotic plaques. This demonstrates a direct biological mechanism.
Treatment trials provide the strongest evidence. When patients take cholesterol-lowering drugs to reduce LDL, their CVD events drop in proportion to how much LDL falls. This is an intervention experiment, not just an observation, so it confirms causation.
Together, these strands meet several Bradford-Hill criteria for causation: strength of association, consistency across studies, dose-response, biological plausibility, and reversibility through treatment.
Examiner InsightWhen asked to evaluate evidence, you must distinguish correlation from causation. State that lifestyle studies alone show only correlation, but genetic evidence and intervention trials provide causal evidence.
Exam TipFor full marks, name at least two distinct types of evidence (e.g. epidemiological data plus statin trials).
Lifestyle Factors and CHD Risk
Three key lifestyle factors significantly reduce coronary heart disease (CHD) risk: diet, exercise, and avoiding smoking each target different parts of the disease process.
Diet affects blood lipids and blood pressure. A diet high in saturated fats raises LDL cholesterol because the liver makes fewer LDL receptors when saturated fat intake is high. Replacing saturated fats with unsaturated fats lowers LDL. Reducing salt lowers blood pressure, and increasing soluble fibre helps remove cholesterol from the gut.
Obesity is a major CHD risk factor, monitored using two indicators.
Body mass index (BMI) is calculated by dividing body mass in kilograms by height in metres squared:
BMI = mass (kg) ÷ height (m)²
| BMI value | Category |
|---|---|
| Below 18.5 | Underweight |
| 18.5–24.9 | Healthy |
| 25.0–29.9 | Overweight |
| 30.0 and above | Obese |
BMI is quick to calculate but does not distinguish fat from muscle. A muscular athlete may register as “overweight” without any health risk.
Waist-to-hip ratio (WHR) is calculated by dividing waist circumference by hip circumference:
WHR = waist circumference ÷ hip circumference
A ratio above 0.85 in women or 0.90 in men indicates increased CHD risk. WHR measures central abdominal fat, which surrounds organs and is more harmful than fat under the skin. Many doctors now consider WHR a better predictor of CVD risk than BMI alone.
Exercise raises HDL, lowers LDL, reduces resting blood pressure, and improves how efficiently the heart pumps blood. Regular aerobic activity also helps maintain a healthy weight.
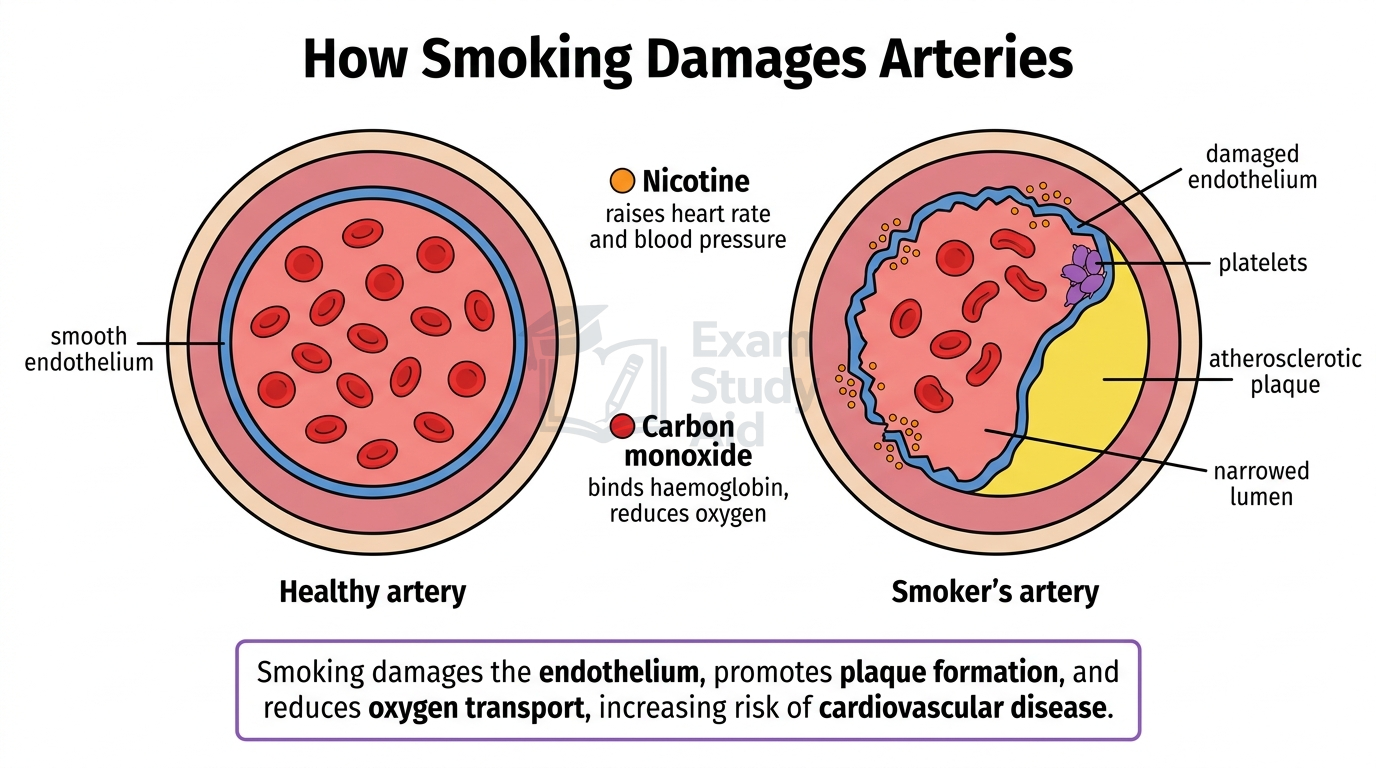
Smoking damages the cardiovascular system in several ways. Nicotine raises heart rate and blood pressure. Carbon monoxide binds irreversibly to haemoglobin, reducing oxygen transport and forcing the heart to work harder. Smoking also damages the endothelium, triggering the start of atherosclerosis.
Treatments for Cardiovascular Disease
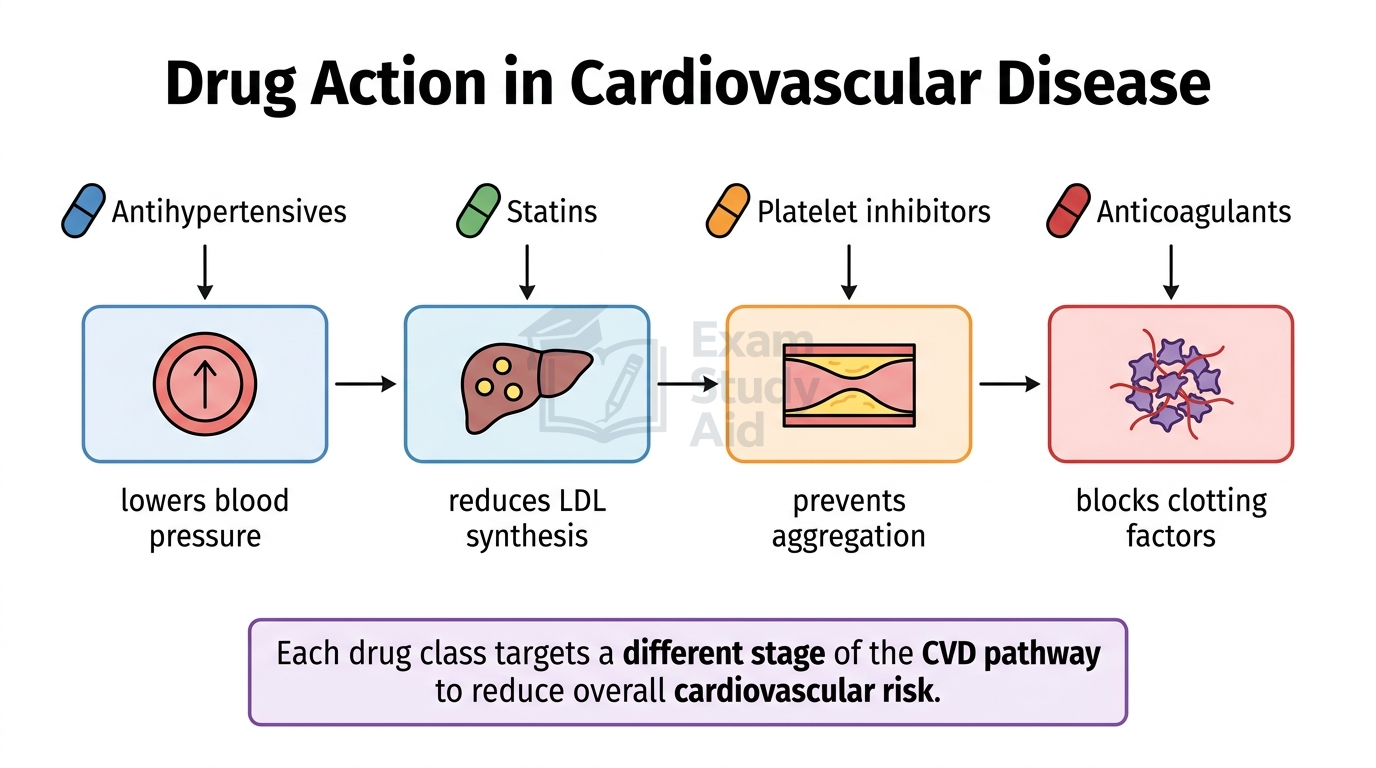
Treatment of CVD uses four main drug classes that target different stages of the disease pathway, with benefits weighed against risks for each patient.
Antihypertensives lower blood pressure to reduce strain on the heart and arteries. They include several types:
- ACE inhibitors block the conversion of angiotensin I to angiotensin II, reducing vasoconstriction
- Beta-blockers slow heart rate and reduce force of contraction
- Calcium channel blockers relax artery walls
- Diuretics reduce blood volume by increasing urine output
| Benefits | Risks |
|---|---|
| Lower blood pressure reduces stroke and heart attack risk | Side effects include dizziness, fatigue, persistent dry cough (ACE inhibitors), and swollen ankles |
Statins lower blood LDL by inhibiting HMG-CoA reductase, the enzyme that controls cholesterol synthesis in the liver. Less cholesterol made means more LDL is taken up from the blood.
| Benefits | Risks |
|---|---|
| Reduce LDL by 30–50% and significantly lower CVD events | Muscle pain, rare cases of liver damage, may need lifelong use |
Anticoagulants (e.g. warfarin, heparin) reduce blood clotting by interfering with clotting factors. Doctors prescribe them for patients at risk of dangerous clots, such as those with atrial fibrillation.
| Benefits | Risks |
|---|---|
| Prevent dangerous clots, strokes and pulmonary embolism | Risk of excessive bleeding from minor injuries; warfarin needs regular blood monitoring |
Platelet inhibitors (e.g. aspirin, clopidogrel) stop platelets sticking together, preventing clot formation in narrowed arteries. They are commonly given after a heart attack.
| Benefits | Risks |
|---|---|
| Reduce risk of further heart attack or stroke | Stomach ulcers and bleeding; not suitable for some asthma sufferers |
When prescribing, doctors weigh up these benefits and risks against the patient’s overall CVD risk. For high-risk patients, the benefits of statins or anticoagulants usually outweigh the side effects.
QUICK RECAP
Key Points
- Cholesterol is a lipid made in the liver and absorbed from animal foods
- Cholesterol travels in blood as lipoproteins because it is insoluble in plasma
- HDL = high protein, low cholesterol; transports cholesterol to liver
- LDL = low protein, high cholesterol; transports cholesterol to tissues
- High HDL is protective; high LDL increases CVD risk
- Total cholesterol below 5.0 mmol/dm³ is healthy; LDL below 3.0
- Evidence for causation: epidemiology, genetics, animal studies, intervention trials
- Bradford-Hill criteria support causation (strength, consistency, dose-response)
- Saturated fats raise LDL; unsaturated fats lower LDL
- BMI = mass (kg) ÷ height (m)²; healthy range 18.5–24.9
- Waist-to-hip ratio above 0.85 (women) or 0.90 (men) indicates risk
- Exercise raises HDL and lowers LDL and blood pressure
- Smoking damages endothelium; carbon monoxide reduces oxygen transport
- Antihypertensives lower blood pressure (ACE inhibitors, beta-blockers)
- Statins inhibit HMG-CoA reductase, reducing LDL synthesis
- Anticoagulants (warfarin, heparin) reduce clotting; risk of bleeding
- Platelet inhibitors (aspirin, clopidogrel) prevent platelet aggregation
- All CVD treatments balance benefits against side effects
CAN I…? PROGRESS CHECK
Self-Assessment
- Can I describe the structure and function of HDLs and LDLs?
- Can I interpret blood cholesterol data and identify CVD risk?
- Can I explain why HDL:LDL ratio matters more than total cholesterol?
- Can I evaluate evidence for the causal link between LDL and CVD?
- Can I distinguish between correlation and causation in CVD studies?
- Can I calculate BMI and waist-to-hip ratio and interpret the results?
- Can I explain how diet, exercise and smoking affect CHD risk?
- Can I describe how each major CVD drug class works?
- Can I evaluate the benefits and risks of statins, antihypertensives, anticoagulants and platelet inhibitors?
- Can I apply this knowledge to suggest lifestyle changes for a high-risk patient?