Learning Objectives
9 objectivesBy the end of this note, you should be able to:
- Understand how DNA replication errors cause mutations through substitution, insertion and deletion of bases
- Recognise that mutations may cause cancer, genetic disorders, or have no observable effect
- Define gene, allele, genotype, phenotype, dominant, recessive, codominance, homozygote and heterozygote
- Interpret monohybrid inheritance patterns and genetic pedigree diagrams
- Explain sex linkage on the X chromosome including red-green colour blindness in humans
- Explain how the cystic fibrosis mutation affects gaseous exchange, digestive and reproductive systems
- Describe genetic screening uses including carrier identification, PGD, amniocentesis and chorionic villus sampling
- Discuss the implications of prenatal genetic screening
- Discuss ethical and social issues of genetic screening from religious, moral and social viewpoints
DNA Mutations and Their Effects
A mutation is a random change in the DNA base sequence that occurs during DNA replication or as a result of external mutagens. DNA polymerase usually proofreads new strands during replication, but occasional errors slip through and become permanent.
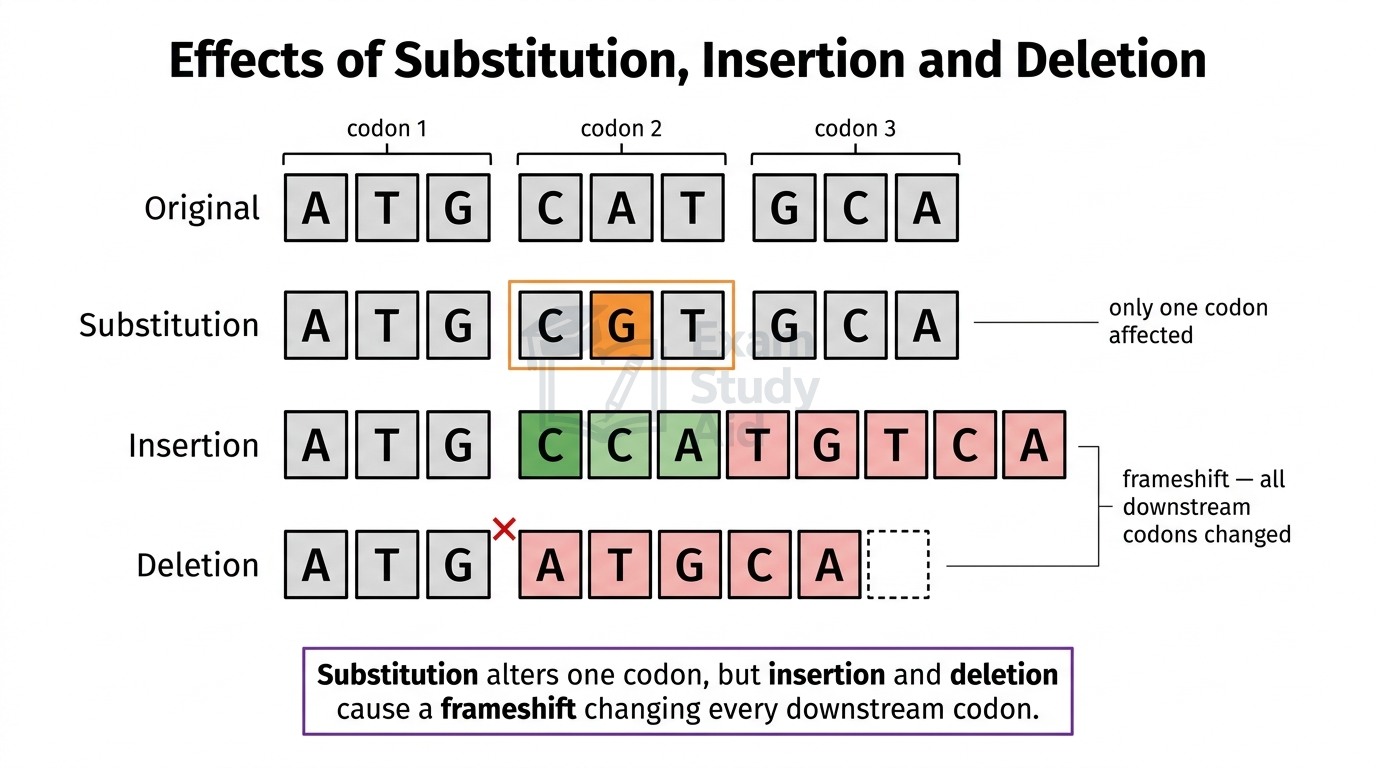
Three types of point mutations affect a single base:
- Substitution: one base is replaced by a different base, for example A swapped for G.
- Insertion: an extra base is added into the sequence.
- Deletion: a base is removed from the sequence.
Substitution affects only one codon, which means at most one amino acid changes. Insertion and deletion are far more disruptive because they cause a frame shift. Every codon downstream of the mutation point is read incorrectly, often changing many amino acids.
The effect of a mutation depends on where it occurs and how it changes the protein produced. Many mutations have no observable effect for several reasons. The genetic code is degenerate, so a substitution may still code for the same amino acid. Other mutations occur in non-coding DNA, which does not code for proteins.
Some mutations cause genetic disorders by producing a non-functional or abnormal protein. Examples include cystic fibrosis, sickle cell anaemia and Huntington’s disease. A small number of mutations cause cancer when they affect genes controlling cell division. Mutations in proto-oncogenes or tumour suppressor genes can lead to uncontrolled cell growth.
MisconceptionStudents often assume all mutations are harmful. In reality, most mutations are silent or neutral because the genetic code is degenerate, or the mutation occurs in non-coding DNA. Only a small fraction cause disease.
Exam TipAlways state that “many mutations have no observable effect” when describing mutation outcomes.
Key Genetic Terms
A gene is a length of DNA coding for one polypeptide, and the variations of that gene found in a population are called alleles.
Each individual has two alleles for every gene, one inherited from each parent. The combination of alleles a person carries is their genotype. The observable characteristic this produces is their phenotype.
The relationships between alleles are summarised below:
| Term | Definition |
|---|---|
| Dominant | An allele that is always expressed when present, even in one copy |
| Recessive | An allele expressed only when present in two copies |
| Codominance | Both alleles are expressed equally in the heterozygote |
| Homozygote | An individual with two identical alleles for a gene (e.g. AA or aa) |
| Heterozygote | An individual with two different alleles for a gene (e.g. Aa) |
A capital letter represents the dominant allele, and a lowercase letter the recessive allele. In codominance, both alleles use capital letters with superscripts. The classic example is human ABO blood groups, where $I^{\mathrm{A}}$ and $I^{\mathrm{B}}$ are codominant in the genotype $I^{\mathrm{A}}$ $I^{\mathrm{B}}$.
Examiner InsightExaminers often deduct marks when students confuse genotype and phenotype. Always specify whether you are describing the allele combination (genotype) or the resulting characteristic (phenotype). Use full allele notation in crosses.
Exam TipWrite “homozygous dominant” or “heterozygous” rather than vague terms like “pure” or “mixed”.
Monohybrid Inheritance and Pedigree Diagrams
Monohybrid inheritance describes how a single gene passes from parents to offspring through alleles separating during gamete formation in meiosis.
Each parent contributes one allele per gene, so offspring inherit one allele from each. A Punnett square predicts the probability of each genotype and phenotype in the offspring.
Example Cross: Cystic Fibrosis Carriers
Cystic fibrosis is caused by a recessive allele (f). A cross between two carriers (Ff × Ff) gives:
| F | f | |
|---|---|---|
| F | FF | Ff |
| f | Ff | ff |
The predicted ratio is 1 FF : 2 Ff : 1 ff (genotype). Three out of four offspring are unaffected (FF or Ff), and one in four has cystic fibrosis (ff).
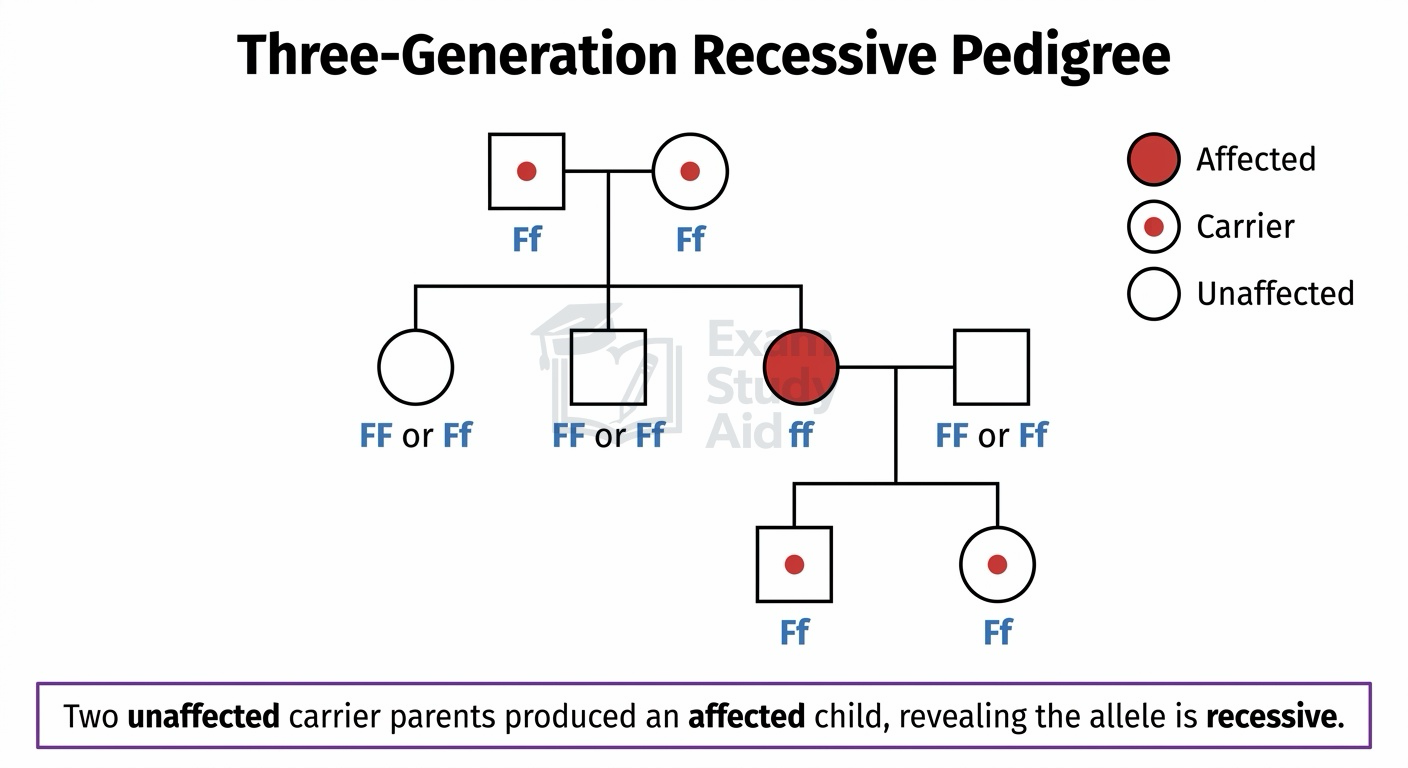
Pedigree Diagrams
A pedigree diagram shows the inheritance of a trait across generations in a family. Standard symbols are used:
- Squares represent males; circles represent females
- Shaded shapes show affected individuals
- A horizontal line between two shapes shows a mating couple
- A vertical line down shows their offspring
- Roman numerals (I, II, III) label generations
To interpret a pedigree, look for clues about whether the allele is dominant or recessive. If two unaffected parents have an affected child, the allele must be recessive. If every affected individual has at least one affected parent, the allele is likely dominant.
Sex Linkage and Colour Blindness
A sex-linked gene is found on one of the sex chromosomes, usually X, and shows different inheritance patterns in males and females.
Females have two X chromosomes (XX), while males have one X and one Y (XY). The Y chromosome is much smaller than X and carries very few genes. This means a male has only one copy of most X-linked genes.
A male needs only one recessive X-linked allele to express the trait. A female needs two copies (one on each X) to be affected. This makes X-linked recessive conditions much more common in males.
Red-Green Colour Blindness
Red-green colour blindness is caused by a recessive allele on the X chromosome. Standard notation uses X^B for the normal (dominant) allele and X^b for the colour-blindness (recessive) allele.
| Genotype | Phenotype | Sex |
|---|---|---|
| X^B X^B | Normal vision | Female |
| X^B X^b | Carrier, normal vision | Female |
| X^b X^b | Colour-blind | Female (rare) |
| X^B Y | Normal vision | Male |
| X^b Y | Colour-blind | Male |
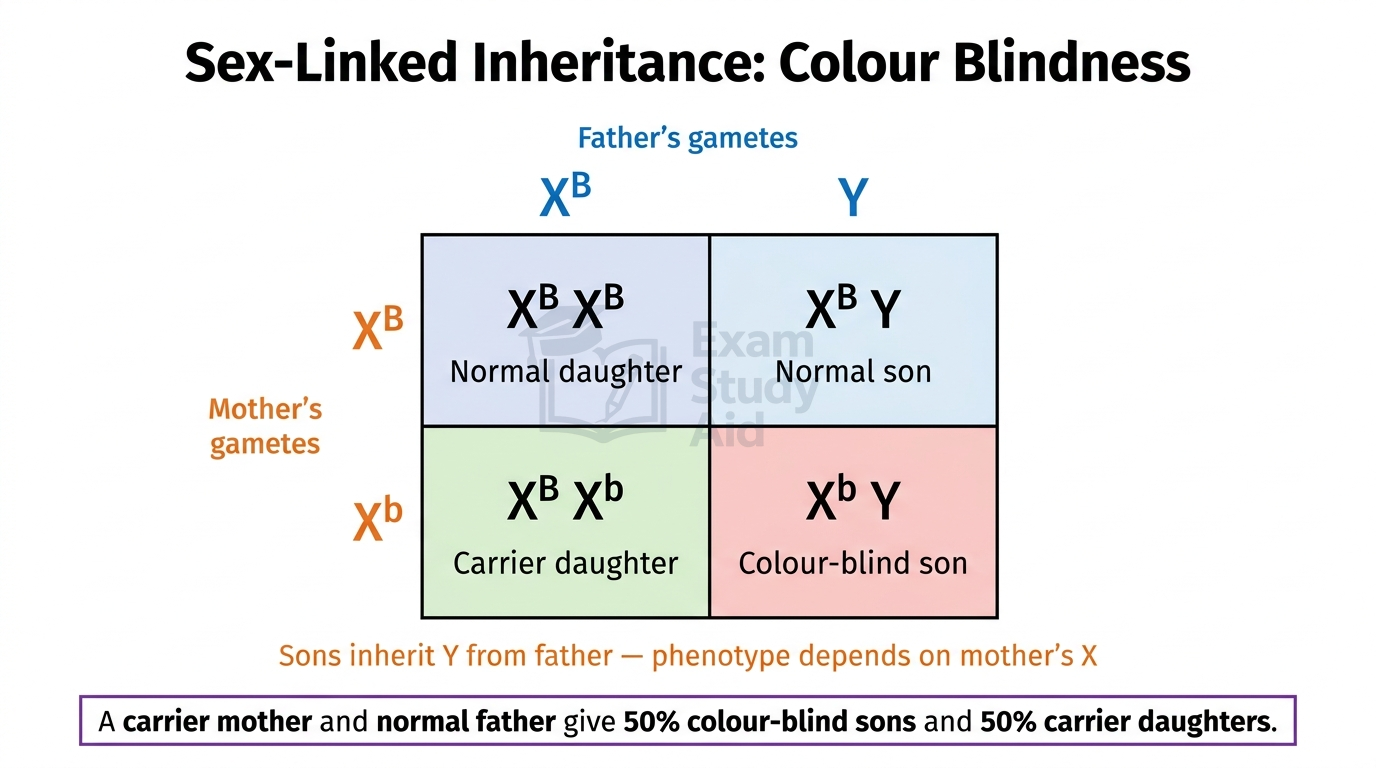
Example Cross: Carrier Mother × Normal Father
The cross is X^B X^b × X^B Y:
| X^B | X^b | |
|---|---|---|
| X^B | X^B X^B | X^B X^b |
| Y | X^B Y | X^b Y |
Daughters are either normal (X^B X^B) or carriers (X^B X^b). Sons are either normal (X^B Y) or colour-blind (X^b Y). Half of the sons are predicted to be colour-blind.
Cystic Fibrosis: Effects on Body Systems
Cystic fibrosis is a genetic disorder caused by a recessive mutation in the CFTR gene located on chromosome 7 in humans.
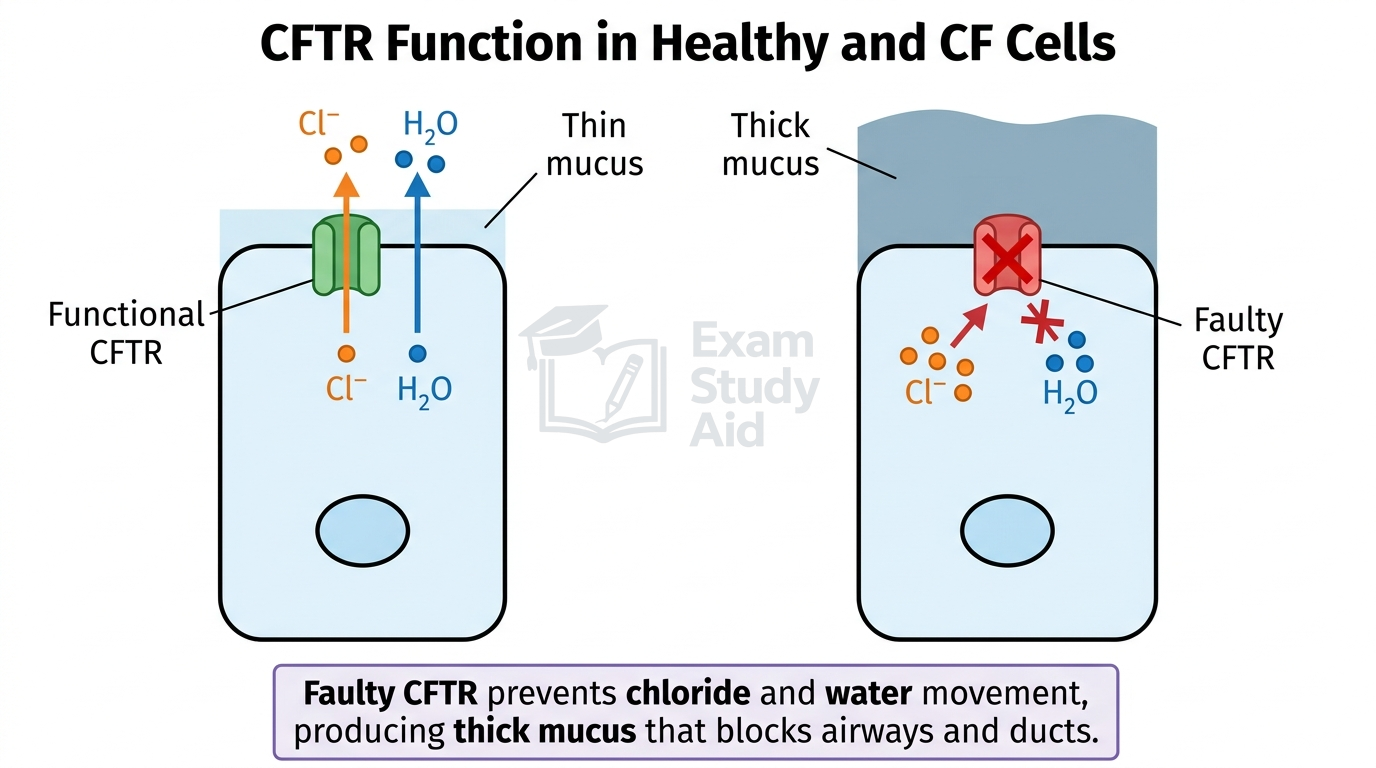
The most common mutation is ΔF508, a deletion of three bases that removes one amino acid (phenylalanine) from the CFTR protein. CFTR (Cystic Fibrosis Transmembrane Regulator) normally transports chloride ions out of cells. Water follows by osmosis, producing a thin watery mucus on epithelial surfaces.
When CFTR is faulty, chloride ions stay inside cells. Less water moves out, so the mucus becomes thick and sticky. This affects three major systems.
Gaseous Exchange System
Thick mucus accumulates in the airways and cannot be cleared by cilia easily. This narrows the airways, reducing airflow and gas exchange. The mucus traps pathogens, leading to repeated lung infections. Over time, chronic inflammation damages alveoli, reducing surface area for gas exchange.
Digestive System
The pancreatic duct becomes blocked by thick mucus. Digestive enzymes such as lipase and amylase cannot reach the small intestine. Food is incompletely digested, so absorption of fats and other nutrients is reduced. Patients often suffer malnutrition and slow weight gain despite eating normally.
Reproductive System
In males, the vas deferens may be blocked or absent due to thick secretions. Sperm cannot reach the urethra, causing male infertility. In females, thick cervical mucus prevents sperm from passing through to fertilise the egg. This reduces fertility but does not always prevent pregnancy completely.
Genetic Screening Methods
Genetic screening is the process of testing an individual’s DNA to identify specific alleles associated with genetic disorders or carrier status.
It allows people to make informed reproductive decisions, but raises ethical questions about how the information is used.
1. Identifying Carriers
A carrier is a person who is heterozygous for a recessive disorder allele and shows no symptoms. Carriers can pass the allele to their children. Adult screening identifies couples where both partners carry the same recessive allele. The couple can then estimate the risk of having an affected child.
2. Pre-Implantation Genetic Diagnosis (PGD)
PGD is performed on embryos created through in vitro fertilisation (IVF). A single cell is removed from an early embryo and tested for specific alleles. Only embryos free of the disorder are implanted into the mother’s uterus. This avoids the issue of terminating an established pregnancy.
3. Prenatal Testing
Prenatal tests are performed during pregnancy to check whether the fetus has a genetic disorder. Two main techniques are used:
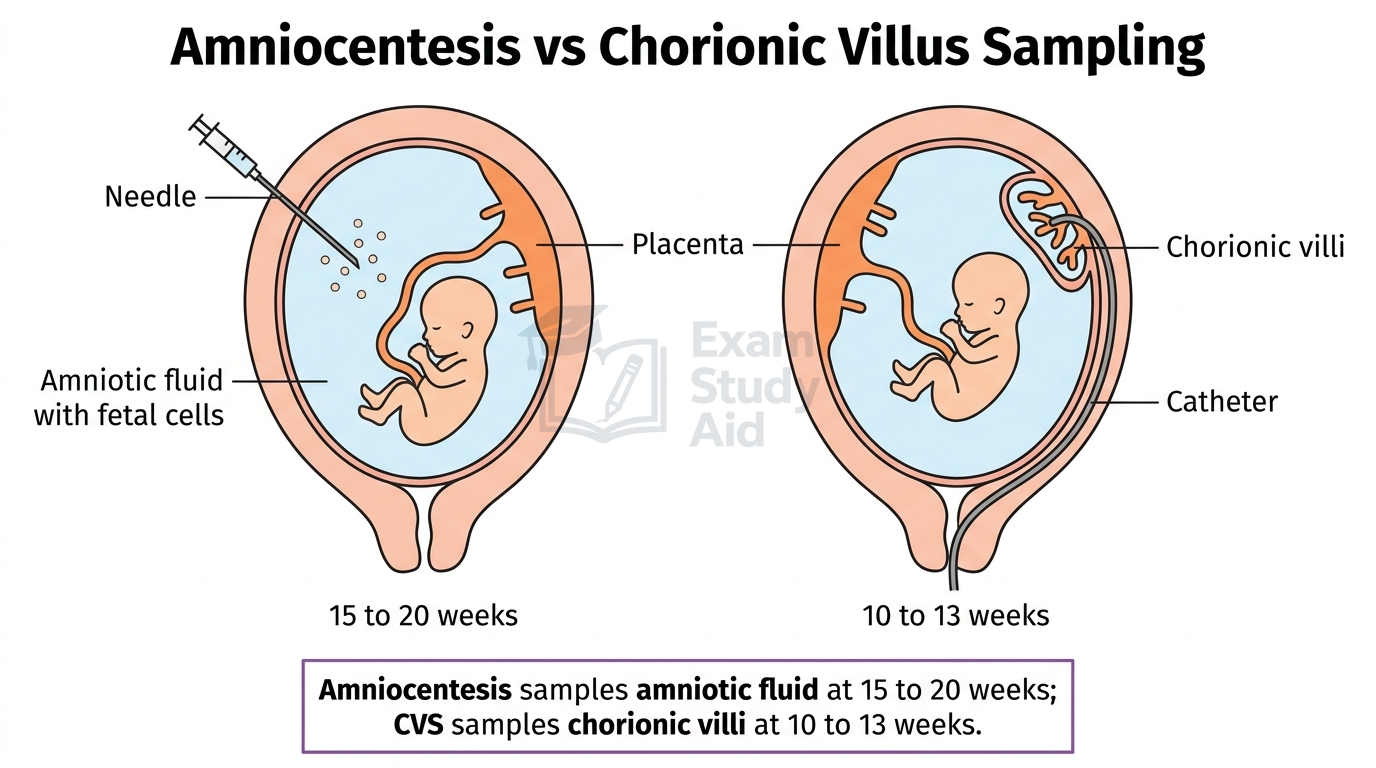
| Test | Timing | Method | Risk |
|---|---|---|---|
| Amniocentesis | 15–20 weeks | A needle removes amniotic fluid containing fetal cells | About 0.5–1% risk of miscarriage |
| Chorionic villus sampling (CVS) | 10–13 weeks | A sample is taken from the placental chorionic villi | About 1–2% risk of miscarriage |
Both tests provide cells whose DNA can be analysed for mutations. CVS is performed earlier than amniocentesis, giving parents more time to make decisions. CVS carries a slightly higher miscarriage risk than amniocentesis.
Implications of Prenatal Screening
Positive results force parents into difficult choices, including whether to continue or end the pregnancy. Both procedures carry a risk of miscarrying a healthy fetus. Some couples may use the results to prepare medically and emotionally rather than terminate.
Ethical Issues in Genetic Screening
Genetic screening raises ethical concerns spanning religious, moral and social viewpoints, with no single universally agreed answer for individuals or societies.
These issues affect individuals, families and society as a whole.
Arguments For Genetic Screening
- Allows informed reproductive choices
- Identifies carriers so couples can plan accordingly
- Affected children can receive early treatment
- Reduces incidence of genetic disorders in the population
- Reduces long-term suffering and healthcare costs
Arguments Against Genetic Screening
- Procedures like amniocentesis and CVS carry a miscarriage risk
- A positive result may lead to termination of an otherwise healthy life
- Results may cause anxiety and emotional distress
- Selective termination may be seen as discriminatory against disability
- Genetic information may be misused by insurers or employers
Religious Viewpoints
Many religious traditions teach that life begins at conception. For these believers, terminating an embryo or fetus is morally equivalent to taking a human life. PGD raises further concerns because unused embryos are typically destroyed. Other faith perspectives accept screening if it reduces suffering or supports informed parenthood.
Moral and Social Implications
Some critics worry about a slide toward “designer babies”, where parents select for non-medical traits. Others fear that widespread screening could increase social pressure to terminate affected pregnancies. This may stigmatise people living with genetic disorders.
There are also concerns about genetic discrimination, where employers or insurers misuse personal genetic data. Equality of access is another concern, since screening is expensive and not always universally available.
Balanced Decision-Making
Genetic counsellors help families weigh the risks, benefits and personal values involved. There is no universal answer; ethical decisions reflect individual beliefs, cultural background and personal circumstances.
Examiner InsightExaminers reward balanced answers covering multiple viewpoints. Always present arguments both for and against screening, and reference at least one religious or moral concern alongside practical and social factors. Avoid one-sided answers.
Exam TipUse phrases such as “however”, “on the other hand”, and “from a religious viewpoint” to structure your discussion.
QUICK RECAP
Key Points
- Mutations are random changes in DNA base sequence
- Substitution swaps one base for another base
- Insertion and deletion cause a frame shift
- Many mutations have no observable effect
- Some mutations cause cancer or genetic disorders
- A gene codes for one polypeptide
- Different versions of a gene are alleles
- Genotype is the alleles, phenotype is the trait
- Dominant alleles are expressed in heterozygotes
- Codominance: both alleles are expressed equally
- Pedigree diagrams trace inheritance through generations
- Two unaffected parents producing affected child indicates recessive
- X-linked recessive disorders are commoner in males
- Cystic fibrosis: faulty CFTR causes thick mucus
- Mucus blocks airways, pancreatic duct, vas deferens
- Genetic screening: carrier testing, PGD, prenatal tests
- Amniocentesis: 15–20 weeks, fluid sample, miscarriage risk
- CVS: 10–13 weeks, placental sample, slightly higher risk
- PGD avoids termination by selecting unaffected embryos
- Screening raises religious, moral, and social concerns
CAN I…? PROGRESS CHECK
Self-Assessment
- Identify and describe substitution, insertion and deletion mutations?
- Explain why some mutations have no effect, while others cause disease or cancer?
- Define gene, allele, genotype, phenotype, dominant, recessive, codominance, homozygote and heterozygote?
- Construct and interpret a Punnett square for a monohybrid cross?
- Read and interpret a genetic pedigree diagram correctly?
- Explain why X-linked recessive conditions are more common in males?
- Describe how the CFTR mutation affects the gaseous exchange, digestive and reproductive systems?
- Distinguish between amniocentesis and chorionic villus sampling?
- Explain how PGD differs from prenatal genetic testing?
- Discuss the ethical and social issues raised by genetic screening from multiple viewpoints?